41 year old male with itching and scaling.
This is online E log book to discuss our patient’s de-identified health data shared after taking his/her/guardian’s signed informed consent. Here we discuss our individual patient’s problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problems with collective current best evidence based inputs. This e-log book also reflects my patient centered online learning portfolio and your valuable inputs on comment box is welcome .
I’ve been given this case to solve in an attempt to understand the topic of “patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations, and come up with diagnosis and treatment plan.
S.Neeraja Reddy
Roll no 125
9th semester
41 year old male resident of choutuppal came with chief complaints of itching and scaling all over the body since 3 months
HOPI
-Patient was apparently asymptomatic 25 years ago ,then he developed scaling on the scalp
also associated with itching sensation.
The scaling then spread from scalp to his face followed by chest abdomen back and lower and upper limbs.
-He consulted dermatologist and was given medication but it didnot reduce.He used the medication for 15 years.
-He also tried ayurveda and homeopathy medications and believed in somefalse assumptions for treatment. He tried ear piercing as the treatment modality.
-There was slight reduction of itching and scaling but there are recurrent episodes by usage of those medication.
-It aggravated in winter.
-7 years ago one day his condition got worsened while he was working as courier agent after exposure to rain so he went to a local rmp where he was treated with Steroids.(Dexmethasone and triamsinalone injection ) Initially he took medication on every alternate day for 12 days.
Itching relieved immediately within 1 hour
Since then for last 7 years he has been visiting the same rmp.
-3 months back he developed infection at the site of injection associated with yellow discharge but reduced spontaneously.
He also had history of weight loss about 15kgs
-He also complained of weakness (pain in the legs unable to stand for long periods)and pedal edema which is of pitting type from 3 months
-7 days ago he went to the doctor in choutuppal from where he got referred to our hospital.
PAST HISTORY:
No history of diabetes, hypertension, asthama, tuberculosis
no history of any previous surgeries
He has a ear piercing done on left ear as he was told that it would reduce his condition.
FAMILY HISTORY
Significant -his maternal uncle have similar complaints
OCCUPATIONAL HISTORY:
He has been changing his works due to his condition.
He first was a delivery person in Hyderabad then due to marriage he had to come to his hometown where he went to various companies but couldn’t tolerate the chemicals due to his condition and rules of the company. He finally started working as a painter since 5 years
PERSONAL HISTORY:
Diet: vegetarian since the last 10 years
Appetite: decreased since the last 3 months
Sleep: inadequate as he stays awake at night due to the itching
Bowel and bladder : regular
Addictions: drinks 90ml of alcohol daily since 15 years, drinks everyday for a few weeks and then discontinues for a while and then starts again.
Consumes 1 packet of tobacco everyday.
MEDICATION HISTORY:
Methotrexate, propysalic ointment, betamethasone, homeopathy and ayurveda since the last 10 years (irregular)
Inj. Dexamethasone/ triamcinolone every 3 months since the last 7 years.
GENERAL EXAMIANTION:
On examination
Patient is conscious, coherent, cooperative went oriented to time place and person
Moderately built and Moderately nourished
Pallor present
No icterus, cyanosis, clubbing, lymphadenopathy, Edema
Vitals:
Temperature:101
BP: 100/70 mm of Hg
Pulse rate: 96
Respiratory rate: 18cpm
GRBS: 96mg/dl
SYSTEMIC EXAMINATION:
1) CVS:
S1 and S2 heard
No thrills and murmurs
2) RESPIRATORY SYSTEM:
Inspection: no scars, equal bilateral chest expansion,
Percussion: resonant in all areas
Palpation: trachea centrally placed, bilateral expansion of chest is equal
Ausculation: vesicular breath sounds heard in all areas
3)ABDOMEN;
flat abdomen, no scars , scaling all over the skin, no hepatomegaly and splenomegaly
No tenderness present
4)CNS:
Normal higher motor functions
No focal neurological deficits
Clinical images
Provisional diagnosis
psoriasis
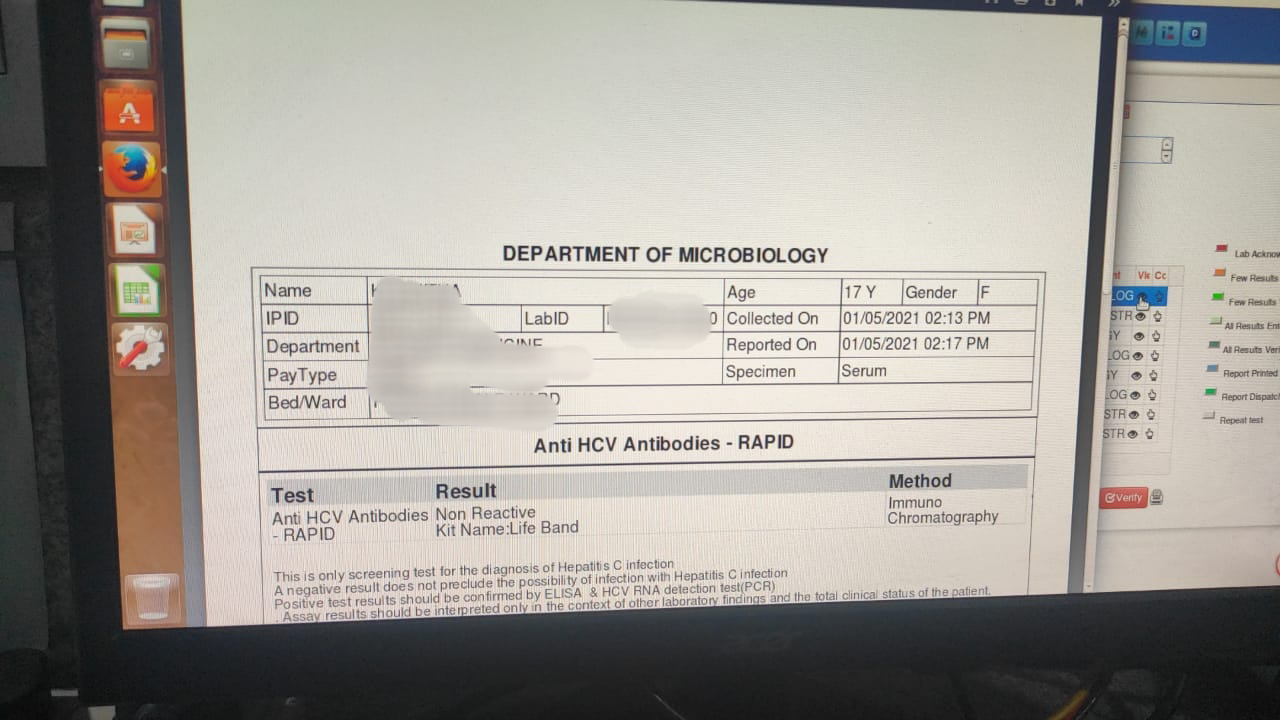
INVESTIGATIONS
LFT
Urinalysis
Chest xray
TREATMENT:1) liquid paraffin+glycerin+water (apply in equal proportions) three times/day
2)tab atarax 25mg OD
3) tab shelcal OD
4)protein x powder with milk
5) high protein diet
6) tab MVT OD
7) tab pregabalin 75mg + tab methylcobalamine 750mcg


















Comments
Post a Comment