65 YEAR OLD MALE WITH SHORTNESS OF BREATH
This is an online e log book to discuss our patient de-identified health data shared after taking his / her / guardians signed informed consent. Here we discuss our individual patients problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problem with collective current best evident based input.
This E blog also reflects my patient centered online learning portfolio.
I have been given this case to solve in an attempt to understand the topic of " patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings investigations and come up with diagnosis and treatment plan.
Icu
HOD-DR.RAKESH BISWAS
PG-DR.KRANTHI
PG-DR PRACHETAN
65 year old male farmer by occupation came with chief complaints of
- Pedal edema since 2 days
- Facial puffiness since 2 days
- Shortness of breath since 2 days
History of presenting illness
-Patient was apparently normal till 2016,
- In 2017,During routine health check up patient was diagnosed with Hypertension and was started on antihypertensive medication by local physician.
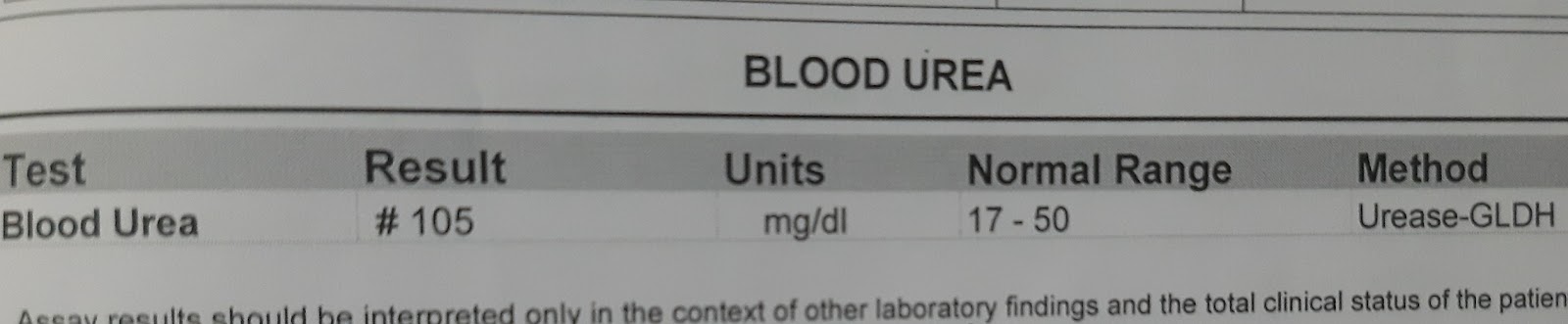
-In 2018 patient had complaints of pedal edema and breathlessness for which he sought for consultation and was diagnosed with chronic kidney disease and was initiated with conservative management.
- He was also advised some dietary modifications which he followed for 1 year.
-He stopped Anti Hypertensive medication as per physicians advice after 2months.
-12 days ago, he had complaints of Shortness of Breath and facialpuffiness went to private hospital in Miryalguda and was advised for dialysis .
He underwent dialysis for 4 times
Course in the hospital
-on 6/7/2023 he developed Bilateral pedal edema pitting type below the knees associated with facial puffiness and Shortness of breath grade 2 MMRC
No aggrevating and relieving factors
Not associated with cough,palpitations, sweating
No H/o reduced urine output,hematuria.
-on 8/7/2023
During dialysis patient developed fever with chills
After undergoing dialysis patient was found hypotensive in the ward,in view of hypotension patient was shifted to ICU.
Vitals at 10 15Am
Bp-60/40 mm hg
PR-136 bpm
RR-29 cpm
Spo2 -97 on RA
Temp 104.4
Fever spikes were present.
Patient BP was 80/40 mmhg ìntra dialysis
Post dialysis patient BP was 60/40 mmhg 300 ml bolus was given.
On 9/7/2023
At around 5 pm patient BP was maintained with noradrenaline
















Treatment:
1.TAB NODOSIS 500MG PO/BD
2.TAB LASIX 40MG PO/BD
3.TAB OROFER XT PO/OD
4.TAB SHELCAL PO/OD
5.BIOD3 PO/OD ONCE A WEEK
6.SYP.POTCHLOR 15ML IN 1 GLASS OF WATER PO/BD


Comments
Post a Comment